The divine punishment of Laocoön and his sons
by two serpents, c. 2nd Century BC
Good health is like an invisible crown which can
only be seen by those who lack it.
(recalled from an unknown source)
The divine punishment of Laocoön and his sons
by two serpents, c. 2nd
Century BC
This page recounts a personal illness case history, along with more general information about the conditions involved. The complex multi-system medical disorder discussed on this page began for me insidiously in 1984. Only in 1986 was it was apparent to me that something significant was going awry with my health, though it would be four more years before I could actually put a label on it.
Although I have used standard and sometimes complex medical terminology which may not always be familiar to lay persons, I have tried to define some of the most important or unusual words below. For a number of reasons, I believe it would be potentially instructive to other patients and to health care professionals for me to give a detailed description of the symptoms and the course of this disorder, and the impact it had on my professional and personal life:
It is hard to decide how to organize and present this complex case, but I will, in an upcoming section, divide it up largely into the various presenting symptoms extending from 1984 to the present (2014). Not all symptoms listed are important as far as causing serious morbidity or impairment, but I list them all to help foster a comprehensive understanding of the scope and multifaceted nature of the syndrome. Where there were positive clinical signs, laboratory or other objective findings, I will mention them. It is my opinion that most of the symptoms listed on this page are (with a few explicitly noted exceptions) all related to a single multi-system disorder that affects, among several others, the immune, nervous, cardiac, muscular, urinary, and skin systems, a disorder that has evolved in me with time, and that has gone by several names. For the most part, I have not included the expected ordinary and unrelated medical events affecting us all, such as respiratory infections and skin lesions, unless I believe there may be a connection. (I have described the impact of this illness on my professional and personal life elsewhere, but some overlap here on this page is unavoidable.)
I compiled an extensive database of medical articles dealing with most aspects of CFS (from its early history up to 2006)—this may be viewed here. It would be undesirable for me to attempt to give an exhaustive discussion of the extensive scientific literature on CFS—there are better and far more authoritative sources of review articles, and I don't claim to have up-to-date information.
As of 2006, I am no longer following the CFS literature diligently. I expect and hope that this page will eventually become outdated by improved knowledge about CFS.
I will mention briefly the treatments I have received, but wish to emphasize the following:
Medical Advice Disclaimer: Although I will always be a physician with an M.D. degree (and as of 2014 am still licensed to practice medicine in the State of Washington), I have not been in active medical practice as a radiologist since 1994, and have not practiced general medicine since 1972, nor do I carry malpractice insurance. I am not in a position to give or imply any direct or specific medical advice about diagnosing or treating any medical illness or condition, including CFS, UAS, and lymphoma. If you are a patient with a seemingly similar or related condition, you must be individually assessed by your own physician(s), and your treatment should be based on your specific circumstances and needs as well as on newer medical concepts, testing, and therapies that undoubtedly will come along after I was evaluated and treated. I am not recommending any specific treatments for you as a patient, only mentioning what did and did not seem to work for me in my own possibly unique circumstances and at the time I was treated.
I cannot avoid the use of medical terminology, some of which may appear unfamiliar and abstruse to lay persons, but I will try to provide brief simplified definitions and acronyms here (in alphabetical order) for the most important terms that I will use and that were current, at least in about 2006. For more exact and complete definitions, and comprehensive discussion of these conditions, standard medical textbooks and review articles found in PubMed are recommended. I have included some conditions that do not apply in my case, but which are often considered in patients with CFS.
The symptoms that I have experienced are listed in the following list in approximately chronological order of their first definite appearance. I have also included briefly how they were evaluated and treated (whether or not beneficial). For some topics, I have offered a few selected speculations and opinions of my own. Of all the symptoms listed, flu-like symptoms, fatigue, weakness, and headache have been the most disabling.
Fibromyalgia (FM, onset c. 1984):
In June 1984, I saw my primary care internist Dr. O (whom I rarely visited) about a complaint of having a peculiar mildly uncomfortable sensation in my hands, mildly declining stamina (noted mainly while jogging), and modest depression (which I related to the painful estrangement of a close relative). My hands did not overtly ache, but just felt strange—a sense of thickness or stiffness not particularly localized to the joints—and I especially noted this sensation while performing radiology special procedures such as angiography.
A medical workup in 1984 by Dr. O with blood and treadmill testing was unremarkable. Serum anti-nuclear antibody (ANA) in 1984 was borderline abnormal (1:20) but was normal later, in 1989, thus no evidence even by 1989 of autoimmune disease was found. My kindly doctor felt that I might be working a little too hard, that I might be a little over-stressed, and, since I was 40 by then, that perhaps I was entering another "season" of my life. Perhaps he felt I might even be experiencing symptoms of a mid-life crisis, and therefore had some adjusting to do. He suggested I read a book called The Seasons of a Man's Life by Daniel J. Levinson (which I bought but did not find time to read). He tried me on the antidepressant Amitriptyline, but it provided no benefit and was terribly sedating, and I soon discontinued it. (Prozac was not introduced into clinical use until about 1988). The ongoing symptoms in 1985 remained fairly modest, the depression gradually lifted, and I had minimal concern by the end of 1985 that anything very serious was going on medically.
In retrospect, the hand symptoms and decline of stamina were the first manifestations of the insidious onset of fibromyalgia (FM) and chronic fatigue syndrome (CFS). I had not had any recent precipitating viral illness that I can recall just before I developed these first symptoms in 1984 (though many CFS patients date the onset of their illness to a viral infection, in which case the condition is sometimes termed postviral fatigue syndrome). Followup standard medical workups by my internist Dr. O performed in 1986 and 1989 were negative despite progressing symptoms. No specific diagnosis was made for these symptoms during 1984 to 1989.
FM symptoms gradually worsened from about 1984 to 1989 to become a generalized burning, uncomfortable feeling primarily affecting the soft-tissues of my limbs and upper torso. It did not always involve all limbs equally—often it was more apparent on the left, the same side in which I developed the greatest weakness and clumsiness (see below). FM symptoms fluctuated, but eventually became present most of the time, were worse when I was fatigued, and most noticeable when I was trying to go to sleep and before arising in the morning. At times there was associated localized muscle and soft-tissue tenderness or skin hyperesthesia or dysesthesia. I also perceived a generalized lowering of pain threshold and/or increased vulnerability to soft tissue injury. For most of the time, however, I have not had objectively demonstrable tender points sufficient in number and/or sensitivity to satisfy the rather arbitrary diagnostic criteria of fibromyalgia syndrome (though I clearly have the symptom of fibromyalgia). FM symptoms gradually blended by c. 1988 with a more generalized flu-like fatiguing illness (CFS, discussed below).
Treatments:
Paresthesias (onset 1986):
I developed mild fleeting peripheral paresthesias in January 1986 consisting of tingling feather-like skin sensations involving my left arm—these gradually extended to involve other extremities over the next few months. They persist to the present (2014) but are not a significant problem. Neurological examinations by several neurologists have never demonstrated any sensory abnormalities, and I have never noted any peripheral sensory deficit. Somatosensory evoked potential testing (SSEP, a specialized neurological test of sensation), was done in December 1988 and was negative. (In retrospect, paresthesias can be, and in my case were, an integral component of CFS.)
Treatments: None. Vitamin B-12 was tried with no benefit.
Motor manifestations (onset 1986):
I developed acute transient left leg paresis (weakness or partial paralysis) in early February 1986, lasting about 20 minutes, presumably of vascular origin in view of the rapid onset and rapid, near-complete clearing of symptoms. My leg, however, never recovered throughout 1986 to previous levels of strength and coordination—I stumbled over it at times, and it felt somewhat clumsy, unsteady, and heavy. Subsequently , I noted a gradual creeping weakness and clumsiness involving my left arm and shoulder and eventually involving all four limbs to some degree. The fluctuating motor clumsiness of my hands was aggravated by physical exertion (for example, when trying to write after performing a strenuous knee arthrogram). I eventually had to give up skiing by 1987, tennis (the sport I truly loved) in about 1988, and other vigorous athletics also in about 1988, as a result of the physical unreliability of my left leg, as well as my developing fatigue. (In more recent years beginning in about 1998, I have resumed playing tennis with my wife and her lady friends at a limited level).
My first neurologist, Dr. P, indicated when I first saw him in January 1987 that he suspected that I had a "myelopathic disorder" (abnormality of the spinal cord), possibly multiple sclerosis. However, no brain or intrinsic cervical spinal cord lesion was found on unenhanced head and neck MRI (in February 1987), or on CT-myelography (performed in October 1987), and examination of the cerebrospinal fluid looking for oligoclonal banding (a test for multiple sclerosis) was essentially normal. (However, repeat cerebrospinal fluid examination in 1990 found equivocal oligoclonal banding, of uncertain significance.)
I also noted the onset of muscle fasciculations, focal spasms, and coarser muscle twitches beginning in 1986, which continue to this day (2014), and are almost always visible, especially in the soles of my feet. A single-fiber electromyogram (EMG, July 1990) was interpreted as negative. My neurologists Dr. P and Dr. C. brushed off these twitches as "benign fasciculations", which carry no apparently worrisome prognostic implications. However, I have been distressed that this widespread, objective, and readily demonstrable manifestation of neurological motor dysfunction was so readily dismissed as unimportant, as I believe that it has clearly been, in myself at least, a component of a more generalized neurological syndrome affecting muscle function, the impact of which has by no means been benign. I predict that someday this relationship between fasciculations and CFS will be better understood, and can only caution neurologists against glibly minimizing findings which they do not fully understand, especially in the context of a multi-system illness presentation. (Without any specific scientific evidence to back it up, I offer my own speculation that this symptom in CFS reflects some type of chronic irritative stimulation of motor units, perhaps by a noxious chemical such as a cytokine or autoantibody.)
I also was found in October 1987 to have a mild but definite spasticity in my left arm and leg by my second neurologist Dr. C. This was confirmed by an especially careful examination by my second neurosurgical consultant, Dr. K, in early November 1987. Unfortunately, this very important and objective finding was later (c. 1988) apparently discounted by my neurologist Dr. C, perhaps because: (1) the asymmetry of findings on physical examination to him had become less pronounced; (2) the myelogram and MRI testing (described below) yielded no useful confirmatory findings; and (3) he may have thought I was a flake, and his overall confidence in the validity of my medical complaints just seemed to wane.
My muscle weakness component can at times be much greater than my more generalized symptoms of fatigue (i.e., weakness may be present even when fatigue is minimal). Such exacerbations specifically of my muscle weakness have been especially apparent following viral upper respiratory infections, and have lasted up to several weeks after the resolution of the infection. The type of weakness I am describing resembles myasthenia gravis, or the weakness of post-polio syndrome or of MS, and has been termed in the past neuromyasthenia. The specific site of the "lesion" in the neuromuscular pathway, of course, remains unknown. (Given the apparently frequent association with viral infections, I speculate that the immune response to the infections triggers the production of toxic substances, perhaps cytokines or autoantibodies formed through molecular mimicry.)
Quantitative Cybex testing of muscle strength and endurance (first performed in 1990 by a PhD physical therapist, Dr. B) has demonstrated apparently significant but varying asymmetries and abnormalities of muscle strength and endurance. Fortunately (for my well-being) or unfortunately (for establishing objective evidence of impairment), these findings have not been consistently reproducible. (In retrospect, these various motor manifestations can be, and in my case were, an integral component of CFS.)
Treatments: A course of oral Symmetrel (in 1988) was not helpful. No effective therapy for weakness has been found, though rest eventually improves it partially.
Neck pain and possible herniated cervical disk symptoms (onset c. 1985 – 1986); lumbar pain (onset c. 1988):
Beginning as early as 1985 and certainly by 1986, I had a mild component of neck pain and minimal and inconstant radicular discomfort radiating to my right suprascapular region (that is, there was occasional pain radiating from my neck to the area of my shoulder above the shoulder blade, in a pattern suggesting a pinched nerve root). Plain X-rays of the cervical spine in early 1986 showed evidence of mild cervical disk disease at C6 – C7. (This would of course have no relationship to a systemic disorder such as CFS or UAS, other than to confuse the situation and make specific diagnosis that much more difficult.) Being only human and worried that there might be a worse alternative explanation such as MS, I was probably seeking in early 1986 a benign mechanical explanation for the various neurological symptoms I was experiencing. I initially ended up seeing in early February a physical medicine specialist, Dr. S, and a neurosurgeon, Dr. M. As there was evidence of cervical disk disease on X-ray, and initially at least some apparently convincing confirmatory neurological physical findings (weak right deltoid and hand extensors, possibly decreased right biceps and brachioradialis reflexes), Dr. M diagnosed a "right C6 radiculopathy"—that is, an impairment from pinching of the nerve exiting on the right from the cervical spine at the C6 – C7 level. He found no abnormalities in my legs, however. He prescribed a course of neck traction which I followed intermittently up to December 1986, with no apparent benefit.
An MRI (February 1987) and a CT- myelogram (October 1987) were done to evaluate for possible MS and to exclude unexpected findings. A herniated (bulging) cervical disk at C6 – C7, with mild indentation of the spinal cord, was demonstrated especially by MRI, confirming the earlier impression by X-ray and physical exam. However, my neurologist Dr. C and a new neurosurgeon Dr. K that I consulted with felt strongly that the leg symptoms I was experiencing could not be explained by the herniated disk in the neck. Dr. K thought that the disk herniation was essentially a red herring, informing me that the leg weakness and systemic symptoms had to have another (and therefore perhaps more ominous) explanation, such as MS.
I still (in 2019) have episodes of neck pain, predominantly manifested by cervical muscle spasm, which is worse after prolonged upright effort and perhaps not related to the herniated disk—I believe this type of pain results from or relates to muscle weakness. In addition, I still occasionally have mild pain radiating to my right shoulder, which is minor. To further confuse the diagnostic situation, I had intermittent right shoulder pain, perhaps an element of rotator cuff injury, but this gradually improved by 2012.
Lumbar back pain has also been a problem for me intermittently since about 1988, including several episodes of moderately severe burning or sharp sacroiliac pain on movement. These episodes have not been specifically evaluated or treated, other than by rest. It is my opinion that they partly reflect the underlying rheumatic autoimmune disorder, but some episodes could simply be ordinary sacroiliac strains or degenerative disk disease. (CT scans beginning in 2004 in fact demonstrate substantial degenerative disk disease at L3-L4 and L4-L5, with mild scoliosis, quite likely explaining some of the lumbar pain.)
Treatments: Cervical traction, physical therapy, Ansaid or other NSAIDs, rest, neck massage, and light exercise all have produced varying but generally quite modest benefit. Surgery for herniated cervical disk was once considered, but has not been thought to be indicated in view of the many other unrelated and more generalized symptoms.
Fatigue and Chronic Fatigue Syndrome (CFS, onset c. 1986), diminished exercise tolerance (onset 1984); malaise and flu-like symptoms (onset c. 1988); episodes of severe exhaustion (onset c. 1990); and evolution to Undifferentiated Autoimmune Syndrome (UAS, by 1990):
At the time of the onset of FM symptoms described above in 1984, I also noted a gradual insidious onset of reduced exercise tolerance (and eventually, increasing fatigue on exertion). This arose during a relatively unchanging pattern of exercise including jogging, tennis, etc. (The fact that the decline came about while my exercising was initially unchanged supports my belief that "deconditioning" from a lack of exercise was not a sufficient explanation for this phenomenon, though it can contribute to such problems in patients who do not or are unable to exercise). Eventually this evolved to significant fatigue at rest by about 1988, fluctuating from mild fatigue to intermittent severe exhaustion and periods of frank prostration and incapacitation by 1990, requiring extensive periods of rest and recovery. In my own case since about 1991, there has been a fairly predictable and recurring variation of intensity of fatigue symptoms during the day, with the worst time of peak symptoms general falling in the mid to late afternoon, and the best time being in the mid morning and to a lesser extent the evening. (However, in recent years since c. 2000, my fatigue seems to be peaking even earlier in the afternoon, as early as noon, and is lasting longer into the late afternoon). There can be striking exacerbation of fatigue by intense cognitive effort, emotional stress, anger, fear, elation, joy, excitement, exercise, or other physical effort. (This pattern leads me to suspect that CFS is associated with a kind of impairment of brain reserve capacity that becomes manifest during increased CNS activity similar to angina, a phenomenon which I have termed neurangina). Since the early 1990s, such symptoms have at times progressed to a profoundly and overwhelmingly sick feeling (generalized burning aching, mental clouding, nausea, headache, burning chest and vague abdominal discomfort, possibly postural hypotension, and prostration). Fatigue symptoms are also exacerbated by alcohol, which I tend to avoid except at bedtime. Sleep is only partially helpful in improving the fatigue—this is termed "non-restorative sleep", a cardinal symptom of CFS. At times, I also have fever-like symptoms, appearing flushed in the face and with my skin feeling hot to other observers, though my measured temperature is usually normal.
Until I self-diagnosed CFS in May 1990, after reading an article in Time magazine on CFS ("Stalking a Shadowy Assailant", 14 May 1990), I had never been given any meaningful diagnosis that could possibly explain the progressively disabling widespread symptoms I was experiencing (and I had not myself previously been aware of the existence or relevance of CFS). The possibility of "Chronic Epstein-Barr Viral Syndrome" was tentatively but astutely raised in October 1989 by a consulting UW neurologist, Dr. S, but this possibility was apparently dismissed by my usual neurologist Dr. C. For one, I had never had infectious mononucleosis, which is caused by EBV. (My subsequent titers, in 1992, of EBV-related antibodies were negative, consistent with my lack of history of EBV exposure, but in any event it was eventually recognized that chronic EBV infection is only rarely the cause of CFS.)
I have also had several episodes of tender anterior cervical lymph nodes ("lymphadenopathy", though without obvious enlargement), usually coinciding with exacerbations of flu-like symptoms. This is of course one of the cardinal symptoms of CFS.
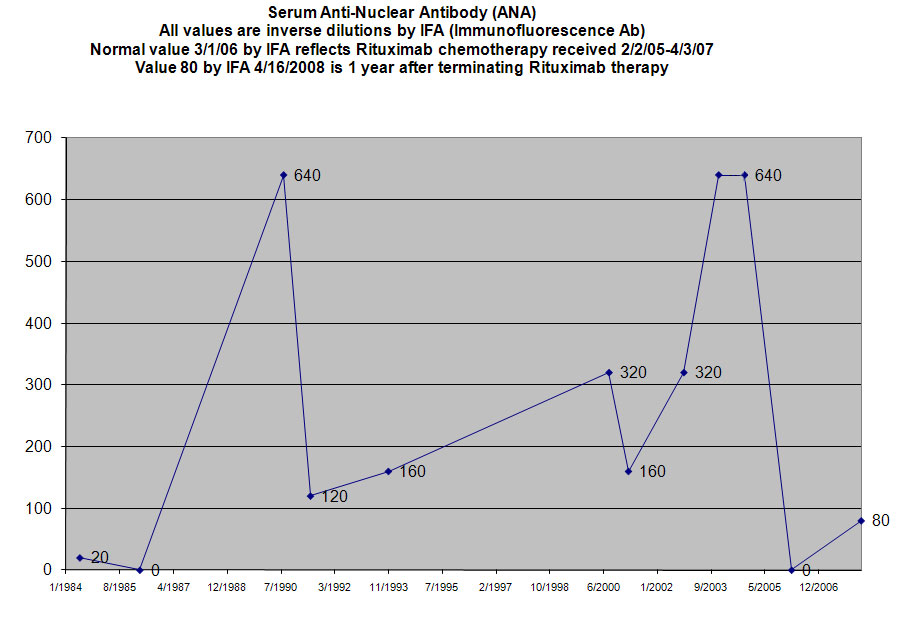
On learning of his interest in CFS, I referred myself to a rheumatologist, Dr. Philip Mease, in August 1990. (At that point, I had formally seen an internist, 3 neurologists, a PM&R specialist, 2 neurosurgeons, 2 urologists, a cardiologist, an ophthalmologist, and a psychiatrist, but remained undiagnosed.) Testing he ordered at that time demonstrated for the first time significant immunological abnormalities, pointing the way to an autoimmune disorder of some type. Specifically, my serum antinuclear antibody (ANA) testing by Immunofluorescent antibody technique (IFA) had by then risen to a clearly abnormal level of 1:640. (It exhibited a "nucleolar pattern", a pattern having limited specificity. Previous ANA by IFA testing at another institution in 1984, 1986, and 1989 had been essentially normal at either 1:20 or "negative".) Serum IgM anticardiolipin antibody was weakly positive at 1:4, and serum complement C3 was borderline abnormal at 154 (normal is 60 – 150). With the positive autoimmune antibodies and consistent symptoms, Dr. Mease made a diagnosis in August 1990 of Undifferentiated Autoimmune Syndrome (UAS), which falls in the spectrum of rheumatic diseases. He acknowledged that I could also be said to have chronic fatigue syndrome, but expressed the view that CFS was a more heterogeneous and poorly recognized diagnostic entity, whereas UAS was a more specific rheumatological diagnosis (and certainly in better repute and less controversial with many physicians). A subsequent rheumatologist, Dr. Steve Overman, changed the emphasis slightly in 2001, saying simply that I met the criteria for both conditions (CFS and UAS), along with incomplete Sjögren's Syndrome. (It is also possible though unprovable that the earlier occurrences of plantar fasciitis in 1979, and subsequently recurring in 1985 and 1999 represented the earliest signs of a systemic autoimmune disorder, which would finally become diagnosable only in 1990.)
Subsequent to the 1990 workup, significantly abnormal serum cytokine values were also demonstrated: Soluble Interleukin-2 Receptor was 1143 U/ml in June 1991 (normal 200 – 750), and 1275 in November 1993. Interleukin-1-Beta was "high" at 32 pg/ml (normal < 4) in October 1992. (Some of these cytokine tests are not normally employed except in research settings, but in my opinion were helfpul to me if giving greater validity and verification of an extensive immune disturbance.)
Repeat ANA by IFA was still abnormal at 1:160 in November 1993 and anti-Double-Stranded DNA was "low positive" at 48 (31 – 60 is "low positive") in November 1993. I continued to have significantly elevated serum ANA by IFA from 1990 (1:160 or above) through 2004, though the titer levels fluctuated as is typically the case. Interestingly, in April 2004, a normal ANA value was obtained using Enzyme Immunoassay or EIA. The ANA by EIA method appears to be less sensitive compared to the ANA by IFA technique, in part because EIA targets only selected nuclear antigens whereas the IFA method inherently targets the entire set of nuclear antigens. This ANA-EIA negative result therefore appeared to me to be a false negative. ANA by IFA can also be falsely negative if not done with great care. According to Mark H. Wener, M.D., Director of the Clinical Immunology Division at the University of Washington, as of February 2006 the Immunofluorescent Antibody or IFA technique remained the standard method of choice for ANA testing at his lab. An ANA titer of 1:640 was subsequently found in September 2004 at the UW lab, using IFA technique, confirming that I still had evidence of pathologically elevated autoimmune antibodies even in 2004 (the year in which my lymphoma was finally diagnosed).
However, in November 2005, my ANA by EIA was again found to be normal. This was probably another false negative, but also by that time I had been on Rituximab chemotherapy for 9 months, and Rituximab can suppress antibody-producing cells including those that secrete ANA. I had the ANA test repeated in March 2006 using the more sensitive IFA method performed at the UW. For the first time since 1989, even this method yielded negative ANA results. Although the negative EIA results might have been due to a false-negative from technical limitations of the test, it appears that even my ANA by IFA had truly become normal by March 2006, presumably reflecting a therapeutic effect of Rituximab therapy. (Regrettably, I did not experience any benefit in CFS/UAS symptoms up to the point of termination of chemotherapy in 2006 despite the normalization of ANA, nor have these symptoms improved as of 2014.) My ANA by IFA has started to climb back up after finishing Rituximab, being 80 in April 2008.
Other more routine blood tests including those for liver, kidney, and thyroid function, etc. have remained normal (to 2014), although by 2008 – 2012 I began showing a borderline high TSH suggesting borderline hypothyroidism (and was placed on oral thyroid hormone supplementation in 2012). In 2012, I also exhibited minor abnormalities of calcium, lipids, and certain other minor blood test abnormalities. The few viral tests I have had (Lyme, EBV) have been negative, except for HHV6 which was positive at a titer of 1:3200 (but a positive test is commonly found in normal persons due to widespread exposure in the general population to this virus).
Treatments:
Urinary symptoms, Interstitial Cystitis (onset c. 1987):
To add to my discomfort, I developed gradual onset of moderate to severe urinary urgency and frequency in 1987, along with mild difficulty urinating (suggesting to me some degree of incomplete sphincter relaxation or spasm). Urinalyses were clear but the initial tentative diagnosis by urologist Dr. A (in January 1988) was "prostatitis" based on a few WBC's in the prostate fluid. Antibiotic and anti-inflammatory medications gave no benefit and the expressed prostate fluid became clear despite continuation of symptoms. Sophisticated urodynamic studies and cystoscopy performed subsequently by urologist Dr. G (in May 1988) were negative, and bladder ultrasound showed no post-void residual urine. My urinary symptoms were only present on standing, and affected my ability to perform prolonged standing radiologic special procedures such as arteriography.
I was told I had interstitial cystitis. This syndrome is apparently not what used to be described as classic interstitial cystitis, as there was no visible inflammation of the bladder wall in my case at least, and its mechanism is not currently well understood. I believe this may be a localized disorder of the urinary sphincter, possibly spasm, or a disorder of bladder sensation (perhaps a sensory misperception arising in the spinal cord). It is, however, a relatively frequent symptom complex accompanying FM and CFS, and I believe it is integral to and one of the protean manifestations of these disorders. Unfortunately, many physicians confronted with a patient having complaints from head to toe and that include the bladder will throw his/her hands up in the air in disgust, muttering that the patient has a "positive review of systems" and begin looking for a psychiatrist to shunt the patient off to.
Treatments: I found no effective therapy, but symptoms have gradually diminished. Ditropan and Imipramine provided no benefit.
Paroxysmal Atrial Fibrillation (PAF, onset 1988):
I had the onset in December 1988, during a stressful night of radiology call, of paroxysmal atrial fibrillation which lasted for 4 hours. I was placed on digoxin then by cardiologist Dr. E and subsequently other anti-arrhythmic drugs. Since 1988, I experienced recurrences of gradually increasing frequency and duration, often arising when I am most symptomatic with fatigue, malaise, and "cytokine stupor". In July 2008, I developed permanent AF which could not be converted back to normal rhythm despite hospital short stays in August and in September 2008 that included oral dofetilide therapy and multiple attempted electrical cardioversions.
PAF at my age of onset is a somewhat unusual condition in the absence of hyperthyroidism, coronary artery disease, alcoholism, or other demonstrable "structural" heart disease. Though it can occur by itself as "lone" atrial fibrillation (i.e., appearing by itself without obvious explanation), in my case I believe, but cannot prove, that its presence was related to my multi-system disorder, and suggests a cardiomyopathic component, clearly not of CNS origin, perhaps viral or humoral/immunological, perhaps reflecting a toxic homeostatic milieu from circulating cytokines, autoantibodies, etc. (One piece of evidence that I believe partially supports this theory: the adjacent graph documents that a somewhat disproportionate number of the onsets of PAF episodes occurred in the mid- to late-afternoon time period from c. 2 PM to c. 6 PM, the time during which my possibly cytokine-induced flu-like CFS symptoms are maximal.)
While hospitalized for intestinal obstruction and lymphoma in 2004, I developed a worrisome episode of rapid ventricular response to PAF, but for the most part the heart rate (ventricular response rate) in the face of PAF has been adequately controlled with cardiac medications.
I also noted an increase in cardiac irritability other than PAF, with frequent episodes of premature contractions, beginning in about 2000. This was treated with the beta-blocking drug metoprolol with some benefit, but the drug was discontinued when sotalol was started in 2004 by cardiologist Dr. D. This type of cardiac irritability increased after 2000, and I frequently developed episodes of bigeminal or trigeminal rhythms which were presumably of supraventricular though undocumented by ECG, often presaging another attack of PAF.
A single episode of amaurosis fugax (transient visual loss in part of the visual field) of the right eye in 2002 led to a duplex Doppler carotid artery ultrasound evaluation for carotid artery disease or patent foramen ovale (done by physiologist Dr. S), but no cardiac shunt abnormality was found. No atrial blood clot or other structural cardiac abnormality was apparent by resting and stress echocardiography (November 2002, done by cardiologist Dr. D). Exercise thallium and sestaMIBI myocardial perfusion scintigraphy in September 2004 were also negative, reducing the likelihood of significant coronary artery disease. (This test was repeated in 2019 again with no positive findings.)
Treatments: (none of these have had much benefit in preventing paroxysmal episodes or chronic AF onset, though some of these drugs effectively reduce the rapidity of the ventricular response and therefore of the heartbeat in response to the rapid atrial contractions):
Cognitive and Neuropsychiatric Symptoms (onset c. 1988):
Before the onset of CFS-like symptoms and UAS, in early 1984, I could probably fairly describe my "premorbid" psychological makeup as follows: I was hard-driving, perfectionistic and rather obsessive-compulsive (not a bad thing in a physician); self-critical; intensely pressured within to succeed in various ways; somewhat introverted; a little high-strung and rather brittle and sensitive to criticism; claustrophobic under certain conditions; somewhat prone to periods of mild depression; and anxious about things that were appropriate to be anxious about. Whatever subtle psychopathologies I might have had lurking in my mental closet, I was a highly functioning and successful physician and a decent family man who was working very long hours with a strong sense of satisfaction regarding my work and career.
In August 1988, I was referred to a psychiatrist Dr. V by my neurologist Dr. C, the latter as it turned out having more-or-less given up on trying to find a straightforward physical explanation for my inexplicable and increasingly exasperating multi-system complaints. I believed at the time that the purpose of this psychiatric consultation was to allow me to seek further support to help me cope with the progressively devastating secondary effects of my undiagnosed illness—in particular, the decline in my ability to perform the full requirements of my job, uphold my family responsibilities, maintain my self-respect, recreate, etc.
In 1988, I had not yet received the diagnoses of either CFS or UAS, though I had been through exhaustive evaluations by numerous physicians. Psychological testing (MMPI, Millon) done by the psychiatrist in 1988 were said to demonstrate tendencies toward obsessive-compulsivity, dysthymia and somatization. However, it is now well-recognized that these standardized psychological tests of personality are incapable of distinguishing CFS-like or multi-system autoimmune disorders from traditional psychiatric disorders, and can be misleading and therefore harmful in this context. Stated another way, the diagnosis of somatoform disorder or somatization is not appropriate in a patient with a multi-system autoimmune disorder. Nevertheless, this type of pseudo-scientific weapon is often wielded by disability insurers against CFS patients. (In a later psychiatric evaluation done for insurance purposes in 2001, at a point when my autoimmune disorder was well-established and somatization was hardly a tenable diagnosis, a psychiatrist Dr. L reviewed with me the criteria required for the diagnosis of dysthymia and concluded that I did not meet these criteria, nor did I qualify for any other persistent substantive psychiatric diagnosis, aside from some appropriate situational emotional responses to job and income loss, etc.)
The psychiatrist Dr. V in 1988, lacking any affirmation from the neurologist Dr. C that a physical disorder was present, was left to conclude that I was depressed, maybe overstressed, maybe "somatisizing", etc. This period of psychotherapy was extraordinarily frustrating and counterproductive for me, in that I knew that I was physically ill but was up against a brick wall in convincing my physicians of this. (I was grateful however that Dr. V was willing to see me after normal work hours, so that I could continue to do my work without interruption. The best that came of these sessions is that he convinced me to overcome my frugal nature and to buy a CD player, as it was obvious to him that I loved music but was reluctant to undertake the expense of upgrading to the newer technology.) I did not know at the time what label to put on my illness, and acknowledged to the psychiatrist that it might not be multiple sclerosis (this initial working diagnosis of my neurologists had been retracted), but I stated that I was absolutely certain that some type of organic illness that had a strong neurological component was present, and that it was causing my declining capabilities. I felt that any depression that might be intermittently present was only an inconstant and secondary component (i.e., a "situational" response). Depression could not possibly explain the most incapacitating symptoms that I was experiencing: severe fatigue and exhaustion, muscle weakness and generalized aching, severe headaches, flu-like symptoms, etc. (I believe, however, that depression can be one of the intrinsic components—though typically only a modest part—of CFS / FM / UAS.) Extended trials of the antidepressants Imipramine (up to 100 mg/day for c. 3 months) and Prozac (20 mg/d for 4 months) were without benefit and produced significant side effects. Subsequent courses of antidepressants Prozac (1990), Protriptyline (1992), Effexor (2001) and Celexa (2001, 2004, and 2011) were also ineffective in relieving any CFS / UAS symptoms.
By 1988 – 1989, I also had noted gradually increasing but fluctuating difficulty with concentration, memory, and complex cognition, as well as marked somnolence (sleepiness) and irritability, all of which were the worst during periods of peak flu-like symptoms, worst in the afternoon. These cognitive symptoms (what I term "cytokine stupor") were aggravated by sleep loss and stress. A trial of amphetamine was prescribed by my neurologist in 1988 but was not helpful and I took it only briefly. Wellbutrin (buproprion, 100 – 150 mg/d), started in 1990, was mildly beneficial in reducing somnolence, though it did not improve any other symptoms and appeared to increase irritability and panic-like symptoms, so I eventually discontinued it. I declined to take Provigil when it was suggested in 2001, due to increasing cardiac arrhythmia problems. I read complex physics books such as Pais's Inward Bound and Subtle is the Lord in 1987, and Kline's Mathematical Thought From Ancient To Modern Times in 1988, but by 1988 was finding that such erudite reading while still working required substantially more mental effort than I might have needed to exert 10 years earlier. This is not to say that I was losing my mind—I just felt that my cognitive depth seemed to have diminished somewhat, and that this could probably not be attributed merely to aging.
I was tried on Doxepin and Ludiomil for my occasional insomnia without success (the former caused lethargy during the daytime), and currently use Benadryl on the rare occasions when I experience prolonged insomnia. I have also found it useful to use a white-noise generating sound machine as a sleep aid.
For the record, I have never used an illegal street drug, have never abused any legal medication, and have never engaged in any form of substance abuse (aside from one evening of alcohol excess in college).
Treatments: Rest when fatigued, stress reduction. Wellbutrin reduced somnolence but no other benefit noted, and I chose to discontinue it. White-noise sound machine has been helpful for improving sleep. Occasional alprazolam or Benadryl helps for initiating sleep. (But caution: benzodiazepine tranquilizers such as alprazolam, though very cheap, can be addictive if taken regularly or abused.) No apparent significant benefit derived from the various anti-depressants and other psychoactive drugs listed above.
Nonspecific Headache (c. 1989):
By 1989, I also developed frequent new nonspecific diffuse bilateral headaches, usually when I was the most symptomatic from CFS. These were clearly different from my past classic migraine with aura (which continue to recur at the usual rate). Rarely, diffuse headache could be the most incapacitating feature of a CFS-like exacerbation. This symptom became significantly less frequent and severe by 2012.
Treatment: Tylenol, Tylenol #3 or Codeine when severe (rarely used), stress reduction, and rest have all been helpful.
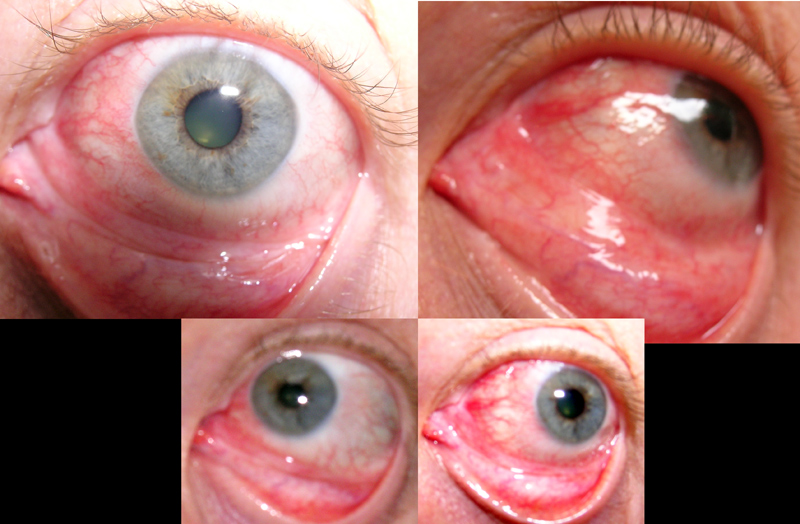
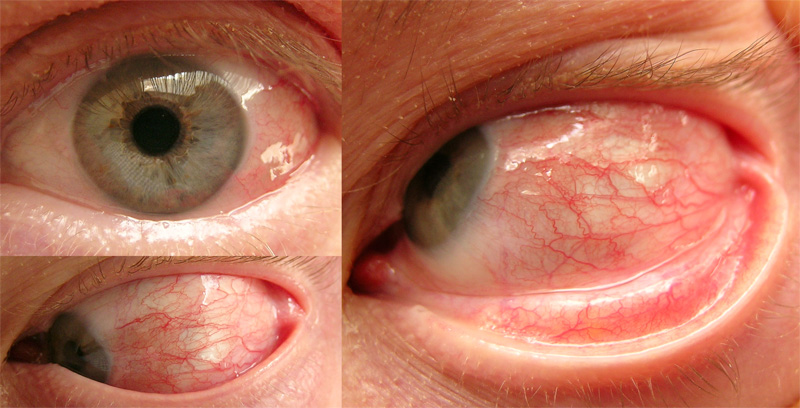
Superficial eye problems and Incomplete Sjögren's syndrome (c. 1991); Recurrent Episcleritis (1994):
In about 1991, I developed a gradually worsening problem of irritated, subjectively dry-feeling eyes with a sensation of grittiness. Schirmer testing, which tests for reduced tear production and was done by my ophthalmologist Dr. J, was initially borderline low at 8 mm in 1991 and 1993, and close to normal at 9 mm in 1994. But eventually this test, repeated in 1997 by a different ophthalmologist Dr. Ch., became overtly abnormal at only 3 mm in the right eye, 7 mm in the left eye, confirming substantial reduction in tear secretion (xerophthalmia). The eye irritation, which continues to the present (2006), has been sufficient to impair sleep at times, and can be quite uncomfortable during the day. A punctal plug, intended to block tear drainage and thereby improve tear retention, was placed in the left eye in February 1999 by ophthalmologist Dr. G. However, it was not helpful and I had my ophthalmologist Dr. Co. remove it in June 2001.
My eye examinations were normal, aside from the issue of tear production, until 1994. Beginning in March 1994, I have experienced several episodes of acute unilateral episcleritis (an inflammation causing redness in part of the white of the eye, treated initially with steroid drops, subsequently with custom-compounded preservative-free steroid drops). I continued to exhibit a low-grade chronic episcleritis (which was treated for a while with Alomide drops in 1994 and Acular PF in 2002, and is less apparent as of 2005). I also developed "3+" punctate keratitis (inflammation of the corneas) in August 1994, causing a frightening clouding of my vision, and which was caused by a reaction to Vasocon-A or Naphcon-A eye drops. These drops contain an antihistamine and decongestant, and I had somehow been left with the incorrect impression by my ophthalmologist that they could be used essentially as often as desired. Fortunately this complication subsequently cleared on discontinuation of the drops. (I believe that my eyes had become by then more vulnerable to hypersensitivity reactions and to injury from irritants such as preservatives like benzalkonium chloride, which is found in most eye drops including alomide and Vasocon-A. Many CFS patients are thought to have hyperactive or "upregulated" immune systems. Preservative-free topical antihistamine or anti-inflammatory preparations for eyes might benefit some patients with CFS or Sjögren's syndrome, but preservatives, as are found in most topical eye drops, and perhaps even the primary drugs themselves, may be more injurious to already compromised corneas.)
Although there was no acute exacerbation at the time, in February 1999 my ophthalmologist Dr. G found that the dye rose bengal, when instilled in my eyes, stained my corneas extensively (as seen by slit-lamp biomicroscopy, especially in the limbic or peripheral region), indicating in this context that the surface layer (epithelium) was chronically injured, perhaps by the abnormally low tear production. (Alternate or additional explanations include hyperconcentration of the tears or the presence of toxic chemicals in the tears, such as inflammatory mediators or cytokines. The latter may be contained in the tears of Sjögren's patients, whose lacrimal glands are often the site of active inflammation.) Thus the findings of keratoconjuncitivitis sicca were established. Later in that year, I returned to Dr. G for what he diagnosed to be an acute unilateral conjunctivitis associated with chemosis (edema of the conjunctiva) and an ulcerated phlyctenule (a superficial inflammatory lymphoid mass)—cultures were negative and he treated me again with steroid drops.
The last attack of episcleritis that I had (as of January 2010) was in January 2009, confirmed by my ophthalmologist Dr. C. He had also noted blepharitis, or more accurately meibomianitis (inflammation of the eyelids and meibomian glands) on several occasions. The meibomian glands produce the oily component found in and essential for healhty tears. This physician, impressed with the inflammatory component in my dry eyes, started me on cyclosporine (Restasis) eye drops in September 2008. I soon noted partial but definite improvement in overall symptoms of keratoconjunctivitis sicca, and my eye examination improved somewhat according to the opthalmologist.
By 1997, my mouth, throat, vocal cords, and trachea had become dryer than normal and produced further distress. Thus I had xerostomia, and combined with the xerophthalmia, it was apparent that I definitely had sicca syndrome and therefore some of the features of Sjögren's syndrome. However, as I lacked (as recently as September 2004) the characteristic autoantibodies used for definitive diagnosis of Sjögren's Syndrome (namely anti-Ro/SSA, anti-La/SSB, or both), I have been said to have "incomplete Sjögren's Syndrome".
Treatments:
Arthralgias (c. 1991):
I have noted gradual development of mild intermittent fluctuating arthralgias (joint pains) mainly in my hands, aggravated by physical use (e.g., yard work, X-ray film handling). My joints also seem more lax and vulnerable to injury. (I have noted above the chronic and recurrent sacroiliac, lumbar, and cervical pain I also continue to experience.) These symptoms, though modest, were I believe a component of my rheumatic disorder, UAS. However as I age, it becomes harder to distinguish symptoms of osteoarthritis from autoimmune rheumatic arthralgias.
Treatments: Ansaid in earlier years, but I wanted to avoid overuse of this drug (which caused gastric symptoms). Oral Glucosamine HCL (1000 mg/d) and Chondroitin sulfate (800 mg/d) begun in 2003 and discontinued in about 2015 probably provided minimal benefit for osteoarthritis (which is unrelated to CFS / UAS). I occasionally talke celecoxib 200 mg for inflammatory pain
Miscellaneous New Symptoms and Signs That May Relate to CFS / UAS:
Though I am still awaiting definitive research on the subject, I believe CFS/ME is at least partly a disorder of the immune system, possibly triggered by other factors such as infection. For five years, I had progressive symptoms consistent with CFS, yet did not have demonstrable autoimmunity, at least as measured by the serum ANA. Beginning in 1990, I developed well-defined evidence of autoimmunity, and was given a new diagnosis, UAS, in addition to the diagnosis of CFS. One might then reasonably ask: Did I have UAS prior to 1990 that simply could not be diagnosed? And if not, was CFS integral to the development of UAS as some kind of precursor condition (which seems likely), or was it entirely unrelated (which seems highly improbable)? For physicians who believe in and accept the validity of UAS but disparage or refuse to make or accept the diagnosis of CFS, was my disorder from 1984 to 1989 unreal before it became indisputably real in the form of UAS?
Subsequently documented in 2004 but probably dating at least as far back as 2000, I developed Follicular Non-Hodgkins Lymphoma, another disorder of the immune system. It is of interest to ask then: At what point in time were the symptoms I was experiencing, that seemed to be arising from CFS / UAS, attributable instead to lymphoma? It seems unlikely, though not impossible, that undiagnosed lymphoma was present as early as 1984, when I first developed the earliest symptoms of fibromyalgia and CFS. In any event, most patients with CFS probably do not have occult lymphomas. The curious scientist-physician in me is inclined to want to tie all these conditions together (just as Einstein tried without success to unite the forces in his Unified Field Theory). My best speculation is that, in me, there were one or more common factors that predisposed to or that precipitated CFS, UAS, and ultimately lymphoma, and that a progression probably occured, perhaps even along a continuum of immune disease. Only time and a great deal more research will tell us for sure if this is the case in other patients, probably long after I am no longer here to explore the interesting details.
Here are some brief points of advice for health care professionals which I wish to emphasize:
(1) Name: The constellation of related symptoms going by the name Chronic Fatigue Syndrome has an unfortunate and trivializing name, but it does have a name and it is a very real medical disorder which causes great distress and impairment. It can be immensely reassuring and helpful to patients (just as it was to me) simply to have a recognized name with which to label the disorder that is disrupting their lives. One should never disparage the usefulness of such a diagnostic entity, even if the etiology and precise nature of the disorder (as with multiple sclerosis in earlier decades) are not well understood.
(2) Belief in Your Patient: If for whatever reason, you cannot bring yourself to believe in the validity and medical significance of CFS (or CFS/ME), you should be honest about it and do yourself and certainly your patients with CFS-like illnesses a great favor: Refer them to a better informed and more compassionate physician. I once saw a busy family practitioner for an immunization. We talked briefly about my medical history, and he seemed to respect my description of my illness, though knowing little about the disorder. Hearing a brief summary of how complex the illness had been for me and how much time I had invested in learning more about it, he asked, "How can a busy doctor like me—who has no time to attend week-long conferences on CFS, and can give maybe 15 minutes max to a patient complaining of CFS-like symptoms—be able to adequately care for such patients?" Regrettably, the answer is that such a physician probably cannot properly care for CFS patients, and should refer them on.
What causes CFS?—it is probably safe to say (at least as of 2014) that the answer is currently not known, and we are still left with mere hypotheses. (Admittedly, I have not kept up on this topic since my lymphoma diagnosis in 2004.) Almost everything about CFS is controversial and subject to ongoing though frustratingly inconclusive research. It is always important to evaluate a patient with apparent CFS for other conditions that can mimic it, but even this seemingly simple concept is controversial in its implementation. The exact evaluation protocol would be determined by a patient's hopefully knowledgeable physician, and would be designed to exclude some of the potentially mimicking conditions (some of which are listed below). Whether depression and other so-called psychiatric conditions are mimics of CFS or simply secondary effects of having a disabling and distressing syndrome remains an unfortunate controversy which can cause great harm to CFS patients. Here are some of the conditions that have at some time been said to predispose to, be associated with, or be alternative explanations for the symptoms of CFS. The items on the list are not mutually exclusive, and some may coexist in the same patient. I have not attempted to evaluate how strong the current evidence is for any condition on this list, though I have listed them in an order reflecting my own biases:
Here are some additional speculative causes of CFS, compiled from undisclosed sources, which I offer to cheer up this discussion:
In 2014, I turned 70, and became an older person. Remarkably, even in 2019, I still have the same fatigue and flu-like symptoms that I began to experience in the 1980s, with no real improvement over this long course. My medical story has been told in detail on this page and on the lymphoma page. Older age can bring on a variety of distressing symptoms, even in the absence of CFS or UAS. Therefore, the age of 70 seems a reasonable cutoff for updating this narrative. Unless I have some dramatic new CFS/UAS development to report, such as a cure by a new miracle drug, "That's all folks".
(1) K Fukuda, SE Straus, I Hickie, MC Sharpe, JG Dobbins,
A Komaroff, "The Chronic Fatigue
Syndrome: A Comprehensive Approach to Its Definition and Study", Ann Int
Med, 15 December 1994, Volume 121 Issue 12, Pages 953-959). This is an
update of the initial CDC definition published by Holmes et al (see below).
(2) Richard A. Gniewek et al, "Comparison of
Antinuclear Antibody Testing Methods by ROC Analysis with Reference to Disease
Diagnosis", Clinical Chemistry 43: 1987-1989, 1997
(3) DC Poskanzer, DA Henderson, C Knuknle, et al,
"Epidemic Neuromyasthenia: An Outbreak in Punta Gorda, Florida", NEJM 257:356, Aug 22, 1957.
(4) ED Acheson, "The Clinical Syndrome Variously Called Benign Myalgic Encephalomyelitis, Iceland
Disease and Epidemic Neuromyasthenia", American Journal of Medicine,
Vol. 26, Issue 4, Pages 569-595, 1959.
(5) I have compiled an extensive database containing more than 5,000 references
on CFS and related conditions. It can be accessed at http://www.mcgoodwin.net/pages/medrefs.html#cfsfmna. This database is no longer being maintained, as of 2006.
(6) The International Classification of Diseases (ICD-10)
of the World Health Organization may be found at http://www.who.int/classifications/icd/en/
(7) GP Holmes, JE Kaplan, NM Gantz, AL Komaroff, LB Schonberger,
SE Straus, JF Jones,
et al "Chronic fatigue syndrome: a working case definition" Ann
Intern Med, 1988 Mar;108(3):387-9. This is the original working CDC
research definition of CFS.
(8) ME/CFS: A Primer for Clinical Practitioners, a publication of the IACFS/ME, 2012 edition.

Page mcgoodwin.net/mcm/mcmabcfsuas.html
Created by Michael McGoodwin
Last update to this page: 2 November 2022
![]()